Amidst the bombardment of COVID news coming every day, how can we evaluate the impact the disease itself has had on New Hampshire’s population and the appropriateness of maintaining a State of Emergency?
Using the number of “cases” is problematic, since case counts are largely driven my mass testing of asymptomatic individuals using an overly sensitive and questionable PCR methodology. In New Hampshire’s recent past, this PCR method has led doctors at Dartmouth-Hitchcock to misdiagnose a whooping cough outbreak in 2007.
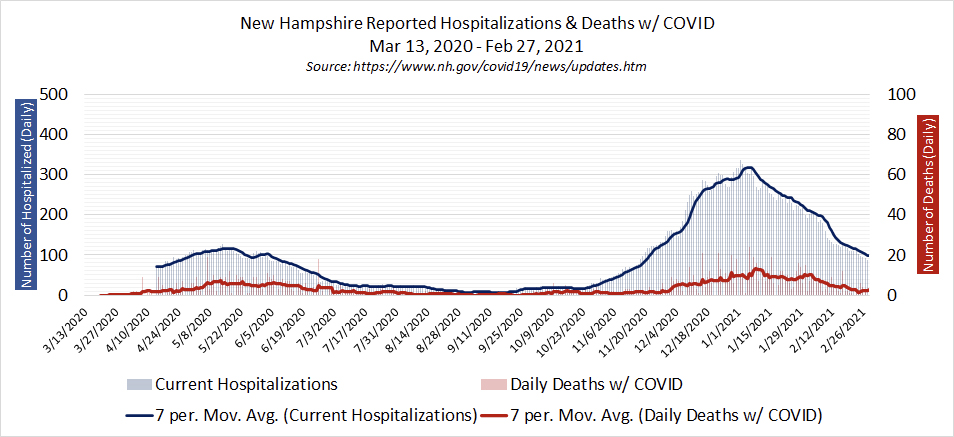
The number of people hospitalized is an important metric to monitor, as concern over hospital capacity was cited by Governor Sununu as a reason for implementing a state of emergency over eleven months ago in March 2020. COVID hospitalizations peaked at 126 (~4% of ~3,100 inpatient beds statewide) in mid-May of 2020, and then receded down to single digits by late summer. Although there was another surge in the fall and winter, COVID hospitalizations peaked at 335 (~11% of hospital capacity) in early January and are now falling fast, down to 87 as of the 2/28/21 report. It should be noted that all throughout, overall hospital capacity in New Hampshire never exceeded 75%. With almost a year of data available, it is clear that hospitals were not, and are not now, at risk of being overwhelmed.
But case counts and hospitalizations both can be exaggerated if based on a very sensitive PCR test. To remove that concern from the equation, one objective metric to gauge the severity of a widespread disease is the total number of people who have died in a given state in a given year. If COVID-19 is a uniquely deadly disease, then that should be apparent in an examination of the overall mortality rate. What does a comparison of the all-cause mortality in 2020 to previous years tells us about the deadliness of COVID-19 to the general population? An examination of New Hampshire’s overall death rate finds that while there was a small increase from the last few years, 2020 was fairly unremarkable compared to recent history.
NH Department of Health and Human Services (DHHS) reports that 805 people died with COVID in New Hampshire in 2020. As of the end of the year, COVID-19 accounts for approximately 5.9% of all 13,583 reported deaths in New Hampshire in 2020 (as of 2/28/21).
To properly compare how many people died over a long period of time, an age-adjustment is used to correct for population and demographic changes. The chart below shows New Hampshire’s overall age-adjusted death rate on an annual basis going back to 1968.
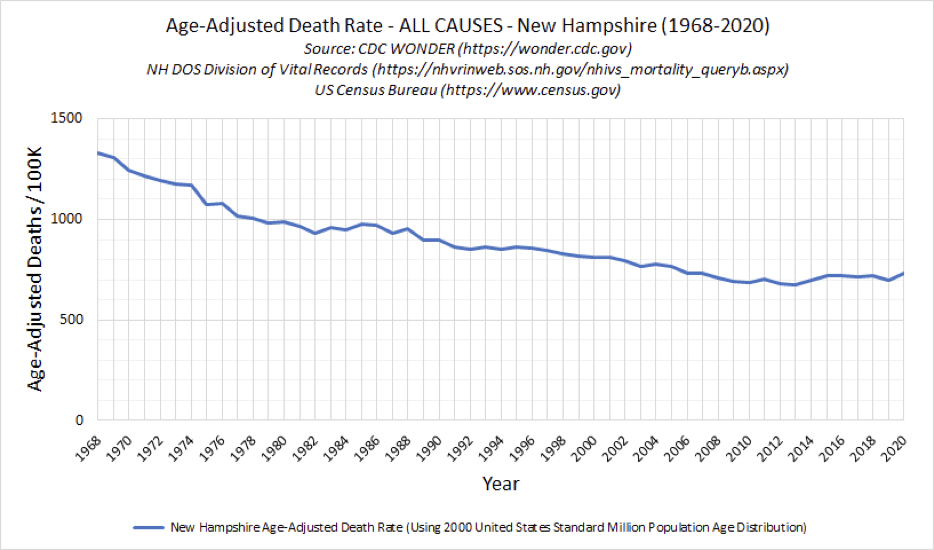
In 1968, which is the earliest date the CDC has easily accessible datasets, the age adjusted death rate in New Hampshire was a little over 1300 per 100K. By the turn of the century it had dropped to about 800 per 100K, and has been between 675 per 100K and 730 per 100K in the last 15 years. This means that death rate has been steadily declining in New Hampshire, as it has across the nation. NH DHHS reported this trend favorably in the 2011 NH State Health Profile. In the more recent past the lowest age-adjusted death rate was in 675 per 100K in 2013, and the last few years it has been steady at about 720, with 2019 being a relatively lower year at 700.
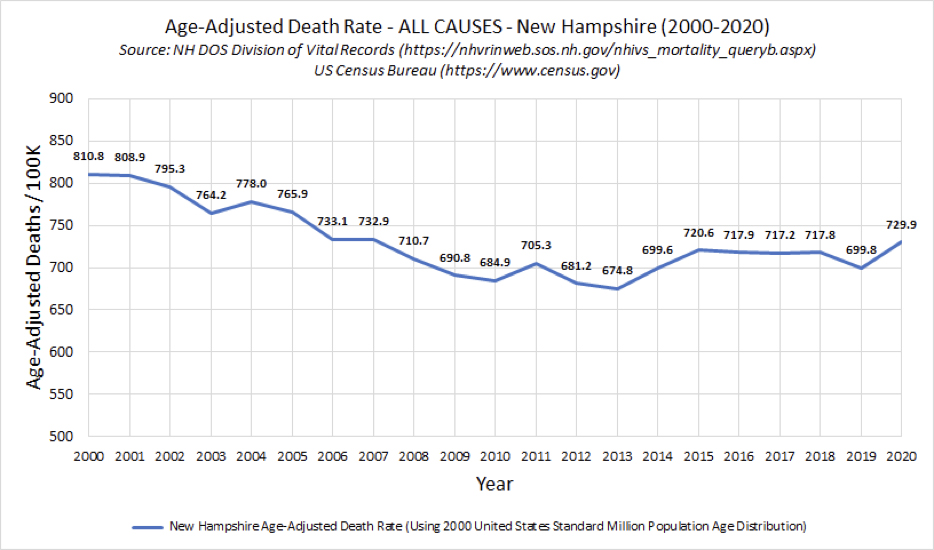
2020 ended up being the 9th highest year of overall deaths in the last 20 years, lower than most of the first decade of the 21st century. When you break down the data into age-specific death rates, a very clear indicator becomes apparent.
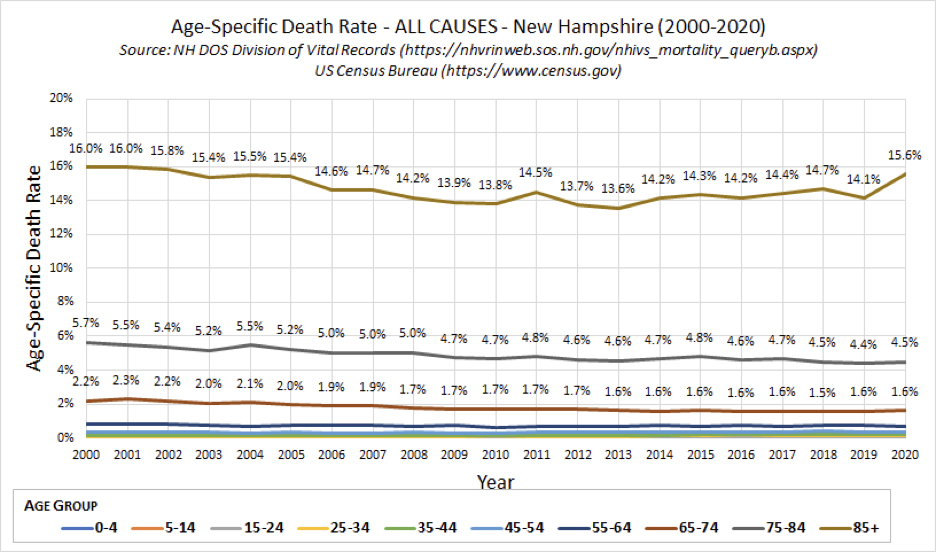
All age brackets showed no discernable change from the last several years except for the age 85+ bracket, which had the highest observed rate since 2002. This makes sense, as NH DHHS reports that 2/3 of all reported deaths with COVID-19 in New Hampshire are from those over 80 years old. In 2019, after having the lowest mortality rate since 2013, the age 85+ population saw an increase from 14.1% to 15.6%. What that means, according to New Hampshire’s own published numbers, is that the overall rate of death for those under age 85 was essentially unchanged in 2020.
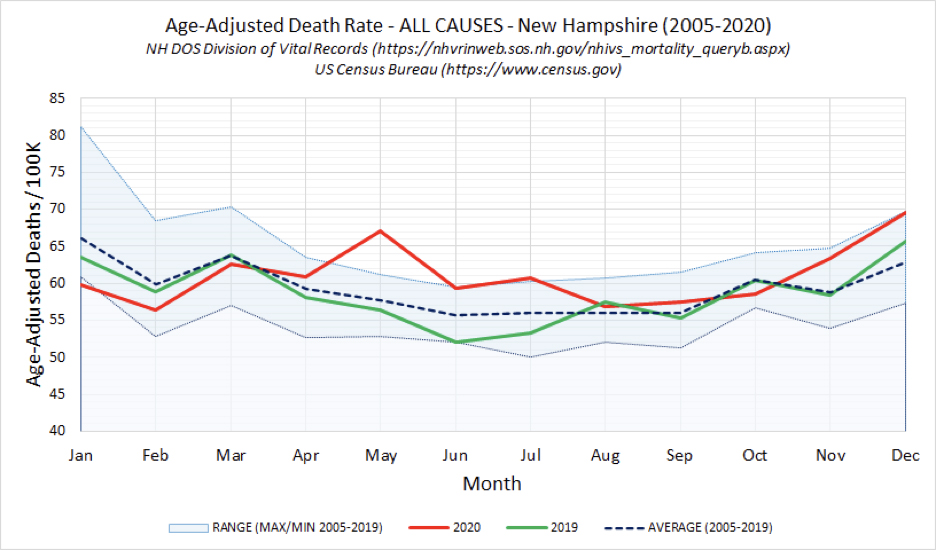
On a more granular level, comparing the all-cause, age-adjusted death rate by month in 2020 to the maximum/minimum range going back 15 years (to 2005) reveals another interesting trend. May 2020 had an abnormally high rate of death above of the maximum observed in the recent past. June and July 2020 were high, but at the maximum range of the recent past. By August 2020 the rate was closer to the average number and stayed there through October 2020. While the rate increased again in November and December 2020, it was still within the range of recently observed experience.
While there will be more statistics and datasets to examine over time, it is clear from the data available eleven months into this State of Emergency that for all but the extremely elderly and those with significant underlying conditions, COVID is not a uniquely fatal disease. And it reinforces the plain observable fact that children are at an incredibly low risk, with not a single recorded COVID death of anyone under the age of 20 in New Hampshire.
For some additional perspective, the 1918-1919 Spanish Flu to which COVID has been compared resulted in the death of about 3,000 Granite Staters between March 1918 and spring 1919. Keep in mind the population of New Hampshire in 1920 was about 443,083, about 1/3 what it is today in 2021.
All this is not intended to downplay the seriousness of a respiratory virus that has claimed the lives of hundreds of Granite Staters over the last year. But we do need to evaluate situations like this, and our response to them, through the lens of history, common sense, and the available health statistics.
In hindsight, did we need a heightened State of Emergency and pages of executive edicts sustained throughout the sunny heat of summer when there was virtually no one contracting, let alone dying from this disease? It doesn’t appear so.
This overall mortality data for 2020, combined with weekly published data from US HHS showing that hospitals in New Hampshire have not been at risk of being overwhelmed, demonstrates that the entire basis for Governor Sununu’s continued State of Emergency is a wrong. There is no argument rooted in science and data that can justify continuing unilateral executive control of every aspect of our lives. We now have real-world data to show us how risky and deadly this disease is to the general population, so we have no excuse to continue to act as if it is still March 2020. The legislature must reclaim their governing authority and put an end to government by executive orders that has gone on for far too long.
James Koniers is Data Analyst for ReopenNH.
Thank you, thank you, THANK YOU!!!!